
The ice bucket challenge is a symbol for much that’s wrong with contemporary charity: a celebration of good intentions without regard for good outcomes. It is iconic for what I call donor-focused philanthropy—making charitable giving about the giver, rather than about those who need help.
In my previous article I mentioned one damaging aspect of donor-focused philanthropy: that it encourages a culture of great praise for small gifts. I believe this culture trades a small short-term gain in donations for a long-term harm by undermining a charitable attitude according to which there are serious problems in the world that desperately need our help, and that won’t be solved by a bucket of ice water. (For those who point to the now $8 million raised, I respond: should we regard the fact that the most widely-publicised fundraising campaign in years has raised 3¢ per citizen, or 0.00006% of GDP, as a cause for celebration or as an indictment of the current state of charitable giving?)
There’s also a second damaging aspect of donor-focused philanthropy: that it regards all causes as equal.
Those who participate in the ice bucket challenge donate to ALS not, seemingly, because they’ve thought about the many problems in the world, and tried to figure out how they personally can best address those problems. Instead, they donate simply because ALS is the originator of the challenge. This is problematic. We should reward the charities that we believe do the most good, not those that have the best marketing strategy, otherwise the most successful charities will be those that are best at soliciting funds, not those that are best at making the world a better place.
ALS is a terrible condition that cruelly cuts short the lives of thousands of people each year, and one for which I desperately hope that we find a cure. But there are very many problems in the world, and there are diseases that affect even more people, harm them to a greater extent, and can be treated at little cost. If we’re not at least having a conversation about this, then we’re not taking seriously the scale and diversity of the world’s ills. Non-profits currently have an immunity card from criticism, responding with indignation if you raise the possibility that some charities might be more effective than others. If we want to solve some of the biggest problems in the world, however, we cannot allow that to continue.
In responses to my previous article, some people claimed that “all causes are equally worthy.” This simply cannot be the case. All people have an equal right to a happy, flourishing life; but some ways of spending money help more people, and help them to a greater extent, than others. This means we need to have a conversation about what the most effective ways of donating are.
How can we compare different charities, even in principle? Within the area of health, economists and ethicists have made particular progress on this issue, developing a metric called the quality-adjusted life-year, or QALY. The idea is that there are two ways in which you can give someone a health benefit: you can extend their life, or you can improve their quality of life. The QALY metric combines those two sorts of benefit. If you can extend one person’s life by one year at full health, that’s one QALY. If you can improve the quality of one person’s life by 50 percentage points for two years, that’s one QALY, too. If you can do this for two people, that’s two QALYs.
This metric is by no means perfect: for example, it ignores the long-term economic effects of programs, and there is room for debate on some of the quality weightings. However, even as a rough measure it allows us to get a sense of the landscape of how much we can benefit people via different health programs.
The drug Riluzole treats ALS by slowing the onset of symptoms, typically extending the patient’s life by three months. It provides one QALY for about $55,000, which is a fairly typical figure for a healthcare program in the US. Because Riluzole is funded by Medicare (including for the under-65 set) and private health insurers, the ALS Association typically does not need to fund it, instead offering other sorts of care. As it acknowledges, this can cost as much as $200,000 per person per year.
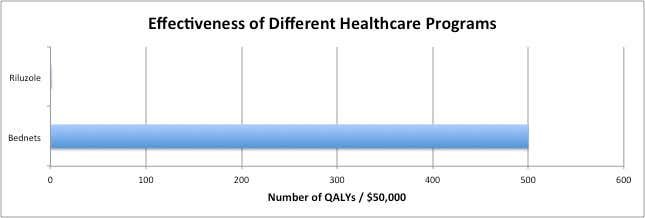
This is expensive, but, given the benefits that care provides, I think that it is an excellent use of money. However, we need to ask: can we do even more good with the same resources? It seems that, by turning our attention further afield, we can. By spending on netting over beds to prevent malaria, that same $50,000 would provide 500 quality-adjusted life years, mainly through the prevention of deaths of children. It would generate five hundred times the positive impact on people’s lives.
In terms of the impact on people’s wellbeing, the difference between donating to antimalarial bednets and donating to ALS is much greater than the difference between donating to ALS and doing nothing at all.
I think that ultimately it’s up to the donor to decide where they give, and the consideration I’ve given above is only one piece of information. But it’s a poor state of affairs where the fact that you can have one hundred times the impact on people’s wellbeing by donating internationally rather than domestically isn’t even recognized or discussed; nor are the relative merits of the ALS association compared to any of the other thousands of charities in the world, each of them honestly doing good work on an important social problem. It does not suggest that people are thinking carefully about their donation decisions. It suggests that we’re rewarding and incentivizing good marketing rather than good work.
The ALS Association does other activities in addition to caregiving, such as campaigning for policy changes, and spending on research. I expect that these will be more effective in the long-run than care and treatment, even though their impacts are more difficult to quantify. But I think that the same is true for research or policy campaigning for malaria, a disease that is more neglected, more tractable, yet greater in scale. If we are to compare like for like, then we should compare research into ALS with research into malaria; again, I think we would conclude that focusing our efforts on malaria would lead to greater total positive impact on people’s wellbeing. Once again, a donor might reasonably disagree with this conclusion, or think that other factors are relevant to their donation decision—we shouldn’t pretend that these choices are easy—but the fact that effectiveness isn’t even discussed when we look at charitable campaigns suggests that we aren’t allocating our donations as well as we could be.
Donor-focused philanthropy neglects to even mention the most important aspect of giving: the impact that your donation has. This isn’t to say that we should be dour and solemn, giving merely out of a sense of duty. In fact the opposite is true: I think that we should be deeply excited about doing good. By virtue of our position as citizens of affluent countries, we have an amazing opportunity to significantly improve the lives of thousands of others at small cost to ourselves. But, if we want to reward the charities that are doing the most good, it’s that ability to help others that we should find exciting, not the number of retweets we can get.