
This item has been corrected.
One of your relatives tests positive for Ebola at a US airport. You’ve watched “Fox & Friends,” so you know this is the end.
However, what is the probability that your loved one does not actually have Ebola even though he tested positive? It is almost certainly higher than 60%, and likely much higher.
The magnitude of false positives for medical tests—a positive test for a condition that a patient does not actually have—is something that is not well understood, even by members of the medical community. We should remember this, as the United States prepares to lock away potential scores of individuals who test positive for Ebola. Many observers do not realize just how many people may spend some time in quarantine when they do not have the dreaded disease.
The cognitive psychologist Gerd Gigerenzer once asked 24 physicians the following hypothetical question, and only two got it right: A test for breast cancer is 90% accurate in identifying patients who actually have breast cancer, and 93% accurate in producing negative results for patients without breast cancer. The incidence of breast cancer in the population is 0.8%. What is the probability that a person who tests positive for breast cancer actually has the disease?
Think you know the answer? Many of the physicians in Gigerenzer’s study said there was a 90% probability that a now-terrified patient flagged for breast cancer is an actual victim of the disease. However, the correct probability is less than 10%.
How? Let’s take 1,000 people from a population in which 0.8% is known to have breast cancer. Eight people in 1,000 actually have breast cancer, and a test that is 90% accurate will rightly identify seven of these eight as suffering from the disease. If eight people in 1,000 have the disease, 992 do not. For 7% of these 992 people, about 70 poor souls, the test will wrongly report the presence of breast cancer.
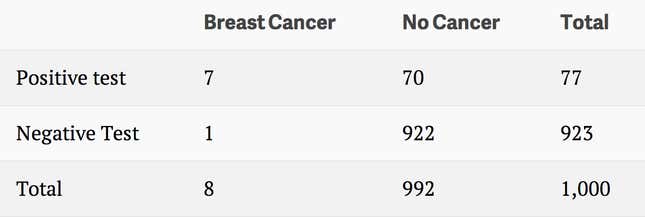
The probability that someone who tests positive for breast cancer actually has the disease is seven in 77, or 9.1%.
Now back to Ebola, to which we can apply the same simple math involving false positives. What is the probability that a person who tests positive for Ebola is actually carrying the virus?
One test that has been suggested for use at US airports is called PCR, or polymerase chain reaction, which can identify Ebola in victims who are not yet symptomatic. The test has a false positive rate of three per 1,000, meaning that for every 1,000 people without Ebola it will wrongly report that three of them have the virus. Not so bad. In patients with Ebola, the test will fail to detect the virus in four of 1,000 people.
Even if we are very liberal in our estimate of how many people in our populations of concern actually have Ebola, say 0.2% or two in 1,000, we will incorrectly report, and perhaps quarantine, a lot of Ebola-free people.
Let’s say we test 1,000 people who arrive in the United States from at-risk countries. Two of them have Ebola and will generate a positive test. Due to the error rate of three in 1,000, three people without Ebola will test positive for the virus.
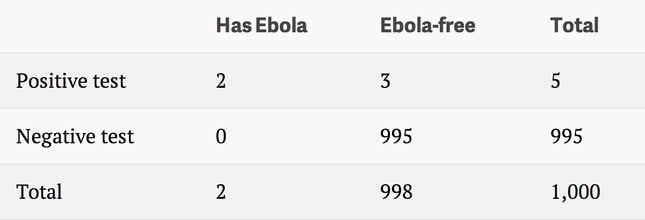
The probability that your relative does not have Ebola, then, is 60%, or three out of five—much better odds than cable news channels would lead you to believe. And since about 50% of people with Ebola do not die, the likelihood that your relative does not have Ebola or has the virus, but survives, is four out of five, or 80%. This is the outcome of a basic misunderstanding of conditional probability; many observers calculate the probability that someone with Ebola will test positive, as some doctors in Gigerenzer’s study did, which is close to 100%. The probability that someone actually has Ebola given that they tested positive is much different.
Of course, the actual rate of Ebola among populations of concern, though unknown, is likely much smaller than one in 500. If the Ebola rate is one in 1,000, your relative has a 75% chance that the positive Ebola test was wrong, and if the rate is one in 10,000, nearly 97% odds of being Ebola-free.
Of the PCR Ebola test, Columbia medical professor Siddhartha Mukherjee wrote in The New York Times (paywall), “One major issue with this kind of rapid-testing quarantine is the phenomenon of false positives. But PCR-based testing for Ebola has a low rate of false positives (three per 1,000).” Yes, most of those with Ebola will test positive, but a vast majority of those who test positive will not have the disease. The issue is not a fleeting “phenomenon,” but a statistical fact.
Quarantining every person who tests positive for Ebola is likely to scare more people to death than the virus itself will claim. Of course, someone who tests red for Ebola will certainly be tested again multiple times to rule out the false positive, but this will likely only be after they have been boxed away for some time.
Mathematician and champion of numeracy John Allen Paulos detailed a false positive problem of conditional probability similar to Gigerenzer’s in his book A Mathematician Reads the Newspaper, writing that “You’ve taken a test for dread disease ‘D’…and your doctor has solemnly advised you that you’ve tested positive. How despondent should you be?” Not very, he concludes.
Some Ebola-watchers may argue that it doesn’t matter how many people are falsely told their lives are over; we must quarantine everyone who tests positive in order to stanch oblivion. If they were familiar with these numbers and were locked away after visiting West Africa, however, they may start to assert their odds.
Correction: A previous version of this post had the incorrect figures for the Negative test in the second table. Gigerenzer’s first name is Gerd, not Max.