15 of history's deadliest pandemics — and what finally stopped each one
From the Antonine Plague to COVID-19 — the pathogens, the death tolls, and the specific conditions that ended each outbreak

Anton Uniqueton / Pexels
Every pandemic in recorded history has ended. This is not a comforting abstraction but a specific historical fact with a specific corollary: each one ended through a specific combination of circumstances — the pathogen mutating to a less lethal form, the population developing immunity through exposure or vaccination, public health interventions reducing transmission, or simply the exhaustion of susceptible hosts. Understanding how pandemics end is not merely academic. It is one of the most practically useful things that history offers.
The pandemics in this list span approximately 2,000 years of recorded human history. They vary enormously in pathogen, mechanism, geographic scope, and death toll — from the Antonine Plague of the Roman Empire to COVID-19, from bubonic plague to smallpox to influenza. What they share is the specific three-part structure that makes each case instructive: a cause (the pathogen and its origin), a spread mechanism (how it moved through the human population), and an ending condition (what specifically brought it to a close).
The endings are often the least understood part of pandemic history. The Black Death did not end because it was defeated; it ended because enough of the European population had died or survived to create a threshold of immunity that slowed transmission below the level required for sustained spread, and because plague's dependence on rat populations and flea vectors created natural limits on its spread that purely human-to-human transmission pathogens do not face. The 1918 influenza pandemic did not end because of any public health intervention; it ended primarily because the virus mutated to less lethal strains and because most of the surviving population had been infected and had some immunity.
These endings are not always satisfying. Several of the pandemics in this list were not ended but subsided — the pathogen still exists, the disease still infects people, and the current quiescence reflects reduced but not eliminated transmission. The distinction between "ended" and "became endemic" is one of the most important in pandemic history, and it applies to several of the cases here.
Antonine Plague (165–180 CE)
Peter Johann Nepomuk Geiger / Wikimedia Commons
The Antonine Plague — named for the Antonine dynasty under whose emperors it occurred — struck the Roman Empire beginning in 165 CE and killed an estimated five million people over 15 years, approximately 10% of the Roman Empire's total population. The Roman army returning from campaigns in the Near East brought the disease westward along the Empire's road network, and the combination of dense urban populations, active military movement, and the Mediterranean trade network ensured its spread throughout the Empire within a few years.
The pathogen has never been definitively identified — no surviving clinical descriptions allow confident diagnosis — but the most commonly proposed candidates are smallpox and measles, based on the symptoms described by the physician Galen, who treated plague victims and left detailed accounts. The death toll and the pattern of spread are consistent with a highly infectious viral disease entering an immunologically naive population with no prior exposure.
The plague ended through a combination of population immunity (survivors and the population born after the first wave had some immunity from exposure) and the natural attenuation that appears to follow a severe initial outbreak — subsequent waves were less deadly than the first. It did not end through any medical intervention; Roman medicine had no specific treatment and no concept of infectious disease transmission. The plague contributed to the political and economic instability of the Roman Empire in the late second century and has been cited by historians as one of the factors in the Empire's eventual decline.
Pathogen: likely smallpox or measles (unconfirmed). Death toll: estimated 5 million. How it ended: population immunity through exposure; natural attenuation of subsequent waves.
Plague of Justinian (541–549 CE)

Josse Lieferinxe / Wikimedia Commons
The Plague of Justinian — the first recorded pandemic of bubonic plague (Yersinia pestis) — struck the Byzantine Empire in 541 CE, beginning in Egypt, spreading through the Mediterranean via grain ships, and reaching Constantinople by 542 CE. At its peak, the plague was killing an estimated 5,000 to 10,000 people per day in Constantinople. The pandemic killed an estimated 25 to 50 million people over approximately eight years, reducing the population of the Mediterranean world by an estimated 25 to 50%.
The plague spread through the same mechanism that would drive the Black Death 800 years later: fleas on black rats (Rattus rattus) carried the Yersinia pestis bacterium, transmitting it to humans through flea bites. The extensive grain storage and trade infrastructure of the Byzantine Empire — which maintained large rat populations at ports, granaries, and along trade routes — provided the vector network through which the plague moved across the Mediterranean world.
The plague subsided after the initial pandemic wave, with subsequent outbreaks occurring periodically for the next two centuries before the disease disappeared from the Mediterranean region around 750 CE. The mechanism of disappearance is debated — hypotheses include the depletion of susceptible rat host populations, climate changes that reduced rat habitats, and the development of some genetic resistance in both rat and human populations. The Plague of Justinian significantly weakened the Byzantine Empire and contributed to its failure to reconquer the western Mediterranean territories that Justinian had briefly recovered.
Pathogen: Yersinia pestis (bubonic plague). Death toll: estimated 25–50 million. How it ended: natural subsidence after multiple waves; rat population dynamics; possible climatic factors.
Black Death (1347–1353)
Pierart dou Tielt / Wikimedia Commons
The Black Death — the most devastating pandemic in recorded human history — killed an estimated 75 to 200 million people in Eurasia between 1347 and 1353, reducing Europe's population by approximately 30 to 60% in a period of approximately six years. It arrived in Europe via Genoese trading ships from the Crimea in October 1347, reaching Sicily first and spreading northward through Italy, France, Spain, England, and the rest of Europe along trade routes with a speed that reflects the density of the medieval European commercial network.
The Black Death was caused by the same pathogen as the Plague of Justinian — Yersinia pestis — but the 14th-century outbreak was significantly more lethal, likely because the European rat and human populations had not been exposed to plague for approximately 600 years and had no residual immunity. The plague spread in three forms: bubonic (transmitted by flea bites, producing the characteristic buboes — swollen lymph nodes), septicemic (bloodstream infection, uniformly fatal), and pneumonic (lung infection, spread directly between humans through respiratory droplets, the most contagious and most deadly form).
The Black Death ended — in the sense that the initial pandemic wave subsided — by approximately 1353, primarily because it had killed or immunized enough of the European population to reduce transmission below the threshold for sustained spread. Plague continued to recur in Europe for the next three centuries, with major outbreaks in 1360, 1374, and the Great Plague of London in 1665, before finally disappearing from Western Europe in the 18th century. The social consequences of the Black Death — the labor shortage that weakened feudalism, the psychological and cultural response to mass death, the collapse of confidence in the Church — reshaped European civilization more profoundly than any other single event in the medieval period.
Pathogen: Yersinia pestis. Death toll: estimated 75–200 million. How it ended: population immunity through mass mortality; recurrent outbreaks for 300 years before permanent subsidence.
Smallpox in the Americas (1520 onward)
Bernardino de Sahagún / Wikimedia Commons
The introduction of smallpox (Variola major) to the Americas by Spanish colonizers beginning in 1520 produced the most catastrophic demographic collapse in recorded history. The indigenous populations of the Americas had no prior exposure to smallpox or any other Old World infectious disease, and their complete immunological naivety made the mortality from smallpox — which typically killed 30% of those infected in European populations with some historical exposure — devastatingly higher, with estimated mortality rates of 50 to 90% in some indigenous communities.
The mechanism of spread was the movement of Spanish colonizers and the subsequent expansion of European settlement across the Americas. Smallpox spread ahead of direct European contact — moving through indigenous trade networks faster than the Europeans themselves — meaning that many communities encountered the epidemic before seeing a European. Hernán Cortés's defeat of the Aztec Empire was substantially enabled by a smallpox epidemic that swept through Tenochtitlán in 1520, killing the Aztec emperor Cuitláhuac and incapacitating much of the city's population.
The epidemic did not end in any conventional sense: smallpox became endemic in the Americas, killing indigenous populations in waves for the next three centuries. The disease was not eliminated from the Americas until the global smallpox eradication campaign of the 20th century, which declared smallpox eradicated in 1980 — the only human infectious disease to have been eradicated through deliberate vaccination and surveillance campaigns.
Pathogen: Variola major (smallpox). Death toll: estimated 25–55 million in the Americas during initial introduction; hundreds of millions globally over centuries. How it ended: global eradication through vaccination (1980).
Cocoliztli epidemic (1545–1550 and 1576–1580)
The cocoliztli epidemic — a term in Nahuatl meaning "pestilence" — struck Mexico in two waves (1545–1550 and 1576–1580), killing an estimated 5 to 15 million people, possibly the majority of the surviving indigenous Mexican population. Combined with the earlier smallpox epidemics and other introduced diseases, the cocoliztli outbreaks contributed to a population collapse that reduced the indigenous population of Mexico from an estimated 25 million before Spanish contact to approximately one million by 1600 — one of the most severe demographic catastrophes in human history.
The pathogen responsible for cocoliztli was unknown until genomic analysis of skeletal remains, published in 2018 in Nature Ecology and Evolution, identified Salmonella enterica serovar Paratyphi C — a cause of enteric fever — in the teeth of burial victims. The identification suggests that cocoliztli was a form of enteric fever, possibly introduced by European colonizers or their livestock, rather than a newly emerged American pathogen. The epidemic's unusual severity may reflect the compound vulnerability of a population that had already been severely reduced and stressed by earlier smallpox epidemics and the disruption of colonization.
The epidemic ended through the exhaustion of susceptible hosts — the population had been reduced so severely that insufficient numbers remained to sustain epidemic transmission. This is one of the grimmer forms of epidemic ending in this list: not immunity, not treatment, not public health intervention, but the near-elimination of the susceptible population itself.
Pathogen: Salmonella enterica (enteric fever), identified by genomic analysis. Death toll: estimated 5–15 million. How it ended: exhaustion of susceptible host population through near-elimination.
Great Plague of London (1665–1666)
-1400x837.jpg)
Credit: Wikimedia Commons (CC BY 4.0)
The Great Plague of London — the last major outbreak of bubonic plague in England — killed approximately 100,000 people in London between 1665 and 1666, roughly 25% of the city's population at the time. The outbreak followed the same mechanism as all European plague outbreaks of the period: Yersinia pestis transmitted through rat flea bites, spreading through the overcrowded, rat-infested conditions of 17th-century London, where sanitation was poor and rats had abundant food supplies in the grain stores and refuse of a growing city.
The public health response to the Great Plague introduced several measures that were genuinely effective at slowing transmission even without knowledge of the causative pathogen or its transmission mechanism: infected households were shut up (quarantined), marked with a red cross, and guarded to prevent movement; the bodies of the dead were buried quickly and at night; and those who could afford to leave London did so, including King Charles II and his court, who fled to Salisbury. The wealthy's flight from the city was documented contemporaneously and became a source of social resentment.
The Great Plague ended through a combination of factors that historians still debate: the depletion of the rat population that sustained the flea-Yersinia cycle, the onset of winter reducing flea activity, the movement of susceptible people out of London, and possibly the Great Fire of London in September 1666, which destroyed large areas of the rat-infested medieval city — though historians are divided on how significant the Fire's role was given that the plague was already subsiding before the Fire occurred.
Pathogen: Yersinia pestis. Death toll: approximately 100,000 in London. How it ended: rat population depletion; seasonal flea inactivity; possible contribution of the Great Fire of London.
Third cholera pandemic (1852–1860)

Prosper Grésy / Wikimedia Commons
Cholera (Vibrio cholerae) killed an estimated one million people in Russia alone during the Third Pandemic and spread through Europe, Asia, Africa, and North America via contaminated water supplies. The Third Pandemic is historically significant not primarily for its death toll — the First and Second Pandemics were similarly deadly — but because it provided the epidemiological evidence that led John Snow to identify contaminated water as the source of cholera transmission in London's 1854 Broad Street outbreak, a landmark moment in the history of epidemiology.
John Snow's investigation of the Broad Street pump outbreak — mapping cholera cases onto a street map of Soho and demonstrating that they clustered around a single contaminated water pump — was the specific event that established the germ theory of disease transmission in practical public health terms, 20 years before Louis Pasteur formally demonstrated the germ theory. Snow's identification of the water source and his persuasion of the local council to remove the pump handle (disabling the contaminated pump) is one of the most cited examples of epidemiological investigation in medical history.
Cholera pandemics continued to occur throughout the 19th century (seven total pandemic waves are recorded from 1817 to the present). The Third Pandemic ended not through a specific medical breakthrough but through the gradual improvement of water sanitation infrastructure in European cities, driven in part by Snow's work and in part by the miasma theory (the then-prevalent belief that disease was spread by bad air), which, while scientifically incorrect, motivated the same sanitation improvements that actually reduced cholera transmission.
Pathogen: Vibrio cholerae. Death toll: millions globally across the pandemic. How it ended: gradual improvement of water sanitation infrastructure in affected cities.
Third plague pandemic (1855–1960)

Credit: Wikimedia Commons (CC BY 4.0)
The Third Plague Pandemic began in Yunnan, China in 1855 and spread globally via steamship, reaching India, Hong Kong, South Africa, the United States (San Francisco, 1900), and South America over the following decades. The pandemic killed approximately 12 million people, the vast majority in India, and persisted in some regions until approximately 1960, making it the longest plague pandemic on record.
The Third Pandemic was significant for the discovery of both the causative pathogen and the transmission mechanism: Alexandre Yersin identified Yersinia pestis as the cause of plague in 1894 during the Hong Kong outbreak, and Paul-Louis Simond demonstrated in 1898 that rat fleas were the transmission vector. These discoveries — made in the middle of an active pandemic — established the scientific basis for plague control and produced the first effective public health response to a plague outbreak based on understanding rather than empirical observation.
The Third Pandemic ended through the combination of rat-flea vector control (killing rats and reducing rat habitat near human settlements), improvements in sanitation that reduced rat populations in ports and cities, and the development of a plague vaccine (though the early vaccines had limited efficacy). Plague was never eradicated — Yersinia pestis persists in wild rodent populations on every inhabited continent — but sustained human transmission was eliminated through vector control.
Pathogen: Yersinia pestis. Death toll: approximately 12 million. How it ended: rat and flea vector control; improved port and urban sanitation; vaccine development.
Spanish flu (1918–1920)
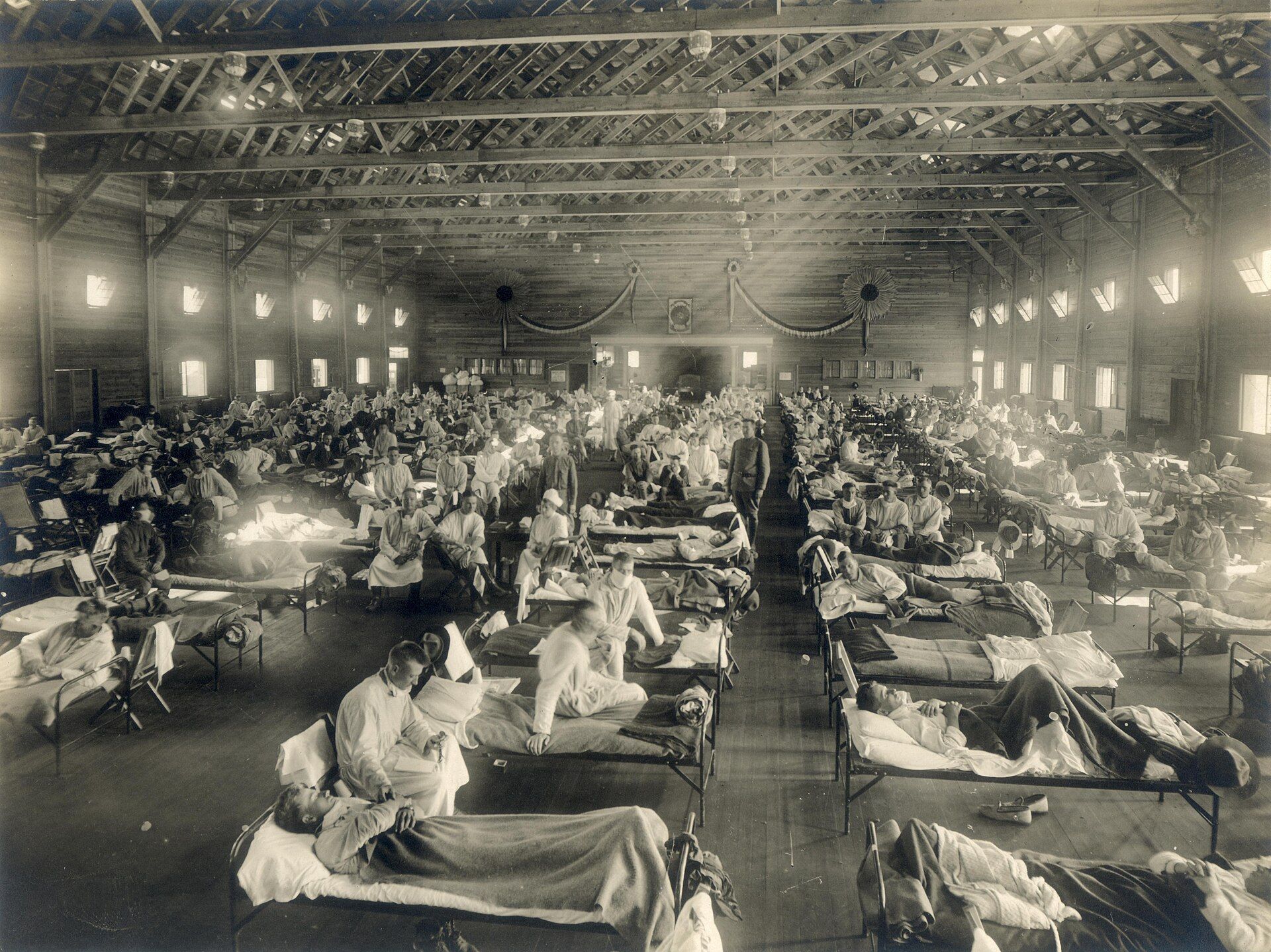
Otis Historical Archives, National Museum of Health and Medicine via Wikimedia Commons
The 1918 influenza pandemic — caused by an H1N1 influenza A virus whose origin is still debated (proposed sites of origin include Kansas, China, and the Western Front) — killed an estimated 50 to 100 million people globally in approximately two years, more than all the combat deaths of World War I. It infected approximately 500 million people — roughly one-third of the world's population at the time — and killed approximately 2 to 3% of those infected, compared to the typical seasonal influenza mortality rate of less than 0.1%.
The Spanish flu had a specific epidemiological characteristic that distinguished it from most influenza pandemics: a W-shaped mortality curve, in which young adults aged 20 to 40 experienced the highest mortality alongside the very young and the very old. The mechanism proposed for this unusual age distribution — that the 1918 strain triggered an especially severe immune response (cytokine storm) in the robust immune systems of young adults — has been debated for a century and remains incompletely understood.
The Spanish flu ended primarily through the development of population immunity through infection. By the end of 1920, most of the surviving population had been infected and had some immunity to the H1N1 strain. There was no vaccine and no effective treatment; the public health responses (social distancing, mask requirements, school closures in some cities) slowed transmission in specific locations but did not end the pandemic. The virus did not disappear — it became endemic as seasonal influenza and eventually evolved into the H1N1 strains that circulate today.
Pathogen: H1N1 influenza A virus. Death toll: estimated 50–100 million. How it ended: population immunity through infection; viral evolution to less lethal endemic strains.
Asian flu (1957–1958)
-600x360.jpg)
Scanpix / Wikimedia Commons
The Asian flu pandemic — caused by an H2N2 influenza A virus that emerged in southern China in early 1957, possibly through reassortment between human and avian influenza strains — killed an estimated one to four million people globally in approximately two years. The pandemic spread rapidly via air travel (faster than any previous pandemic, reflecting the growing commercial aviation network of the late 1950s) and produced a second wave in winter 1957–1958 that was more severe than the initial outbreak.
The Asian flu pandemic was the first pandemic in which the available virological technology allowed rapid identification of the causative strain and the development of a vaccine within months of the pandemic's emergence. The influenza vaccine developed in 1957 was not available in time to prevent the initial pandemic wave but contributed to the management of subsequent waves and the overall lower mortality compared to 1918.
The pandemic ended through the same mechanism as the Spanish flu: population immunity through infection combined with vaccination of at-risk populations. The H2N2 strain circulated as seasonal influenza until 1968, when it was replaced by the H3N2 strain of the Hong Kong flu pandemic. H2N2 has not circulated in humans since 1968, making the current global population — particularly those born after 1968 — completely immunologically naive to it, a potential pandemic risk that influenza surveillance programs monitor.
Pathogen: H2N2 influenza A virus. Death toll: estimated 1–4 million. How it ended: population immunity through infection and vaccination; viral replacement by H3N2 in 1968.
HIV/AIDS pandemic (1981–present)

MONUSCO Photos / Wikimedia Commons (CC BY-SA 2.0)
The HIV/AIDS pandemic — caused by the Human Immunodeficiency Virus (HIV), a retrovirus that destroys CD4+ T cells and progressively impairs immune function, leading to AIDS (Acquired Immunodeficiency Syndrome) — has killed approximately 40 million people since it was first identified in 1981 and continues to infect approximately 1.5 million new people annually. It has not ended; it is the only pandemic in this list that is ongoing in a sustained global sense.
HIV originated in central Africa through cross-species transmission (zoonosis) from chimpanzees — the chimpanzee version of the virus, SIV (Simian Immunodeficiency Virus), crossed into the human population at least twice in the early 20th century, most significantly around Kinshasa (in what is now the Democratic Republic of Congo) in the 1920s. The specific conditions that drove the initial spread — the growth of Kinshasa as a colonial city, the expansion of commercial sex work, medical injection campaigns using reused needles — have been identified through phylogenetic analysis of the earliest HIV strains.
HIV has not ended because no sterilizing vaccine (one that prevents infection) has been developed, because the virus mutates rapidly and integrates into the host genome (making it impossible to eliminate from already-infected cells), and because effective treatment (antiretroviral therapy, introduced in 1996) suppresses the virus to undetectable levels and prevents transmission but does not cure infection. The pandemic has been substantially controlled in high-income countries through antiretroviral therapy and prevention programs, but continues to drive significant mortality in sub-Saharan Africa.
Pathogen: Human Immunodeficiency Virus (HIV). Death toll: approximately 40 million to date; ongoing. How it has been managed (not ended): antiretroviral therapy; prevention programs; ongoing vaccine research.
SARS (2002–2003)

Sparktour / Wikimedia Commons (CC BY-SA 4.0)
Severe Acute Respiratory Syndrome (SARS) — caused by a coronavirus (SARS-CoV-1) that emerged in Guangdong Province, China in late 2002 — infected approximately 8,098 people across 29 countries and killed 774 (a case fatality rate of approximately 9.6%) before being contained within approximately eight months of its international spread. SARS is the pandemic in this list that was most clearly ended by public health intervention rather than by population immunity or viral attenuation.
SARS spread primarily through hospital settings — the majority of cases were healthcare workers and hospital patients — and through the specific superspreader events that characterized its transmission: a single infected physician who stayed at the Metropole Hotel in Hong Kong in February 2003 seeded outbreaks in Hong Kong, Vietnam, Singapore, Canada, and Ireland through the guests who shared his floor. The Metropole Hotel cluster is one of the most studied superspreader events in epidemiology.
SARS was contained through aggressive isolation of confirmed and suspected cases, quarantine of contacts, and hospital infection control measures — the classical public health toolkit applied with unusual speed and thoroughness. The low total number of cases (8,098 globally) reflects both the effectiveness of the containment response and the relatively low transmissibility of SARS-CoV-1 compared to SARS-CoV-2 (COVID-19): SARS-CoV-1 was less contagious and became contagious only after symptoms appeared, making case identification and isolation feasible in a way that was not possible with the pre-symptomatic transmission of SARS-CoV-2.
Pathogen: SARS-CoV-1 (coronavirus). Death toll: 774. How it ended: case isolation and contact quarantine; hospital infection control; superspreader event containment.
West African Ebola epidemic (2014–2016)

Centers for Disease Control / Wikimedia Commons
The West African Ebola epidemic — caused by Ebola virus (Zaire ebolavirus) and centered in Guinea, Sierra Leone, and Liberia — infected approximately 28,616 people and killed 11,310 between 2014 and 2016, making it by far the largest Ebola outbreak in history. Previous Ebola outbreaks had been confined to remote rural areas and had burned out quickly; the 2014 epidemic spread to densely populated urban areas including the capitals of all three affected countries, fundamentally changing the scale and complexity of the response.
Ebola spreads through direct contact with the bodily fluids of infected people, which limits its transmission compared to airborne diseases but makes healthcare settings and traditional burial practices (which involve direct contact with the deceased) significant transmission vectors. The specific features of the 2014 epidemic that drove its unusual scale were the urban spread, the weak health infrastructure of the affected countries, and the initial delayed international response — the outbreak was notified to the WHO in March 2014 but the international response did not scale to meet the epidemic until late 2014.
The epidemic ended through a combination of community engagement that changed burial practices, aggressive contact tracing and isolation, strengthened healthcare worker protection, and the deployment of an experimental Ebola vaccine (rVSV-ZEBOV) that showed high efficacy in a ring vaccination trial and was used to protect healthcare workers and contacts of confirmed cases. The epidemic was declared over in January 2016. The vaccine developed during the 2014–2016 epidemic has since been formally approved and has been used in subsequent Ebola outbreaks in the DRC.
Pathogen: Zaire ebolavirus. Death toll: 11,310. How it ended: contact tracing and isolation; changed burial practices; experimental ring vaccination.
COVID-19 (2019–present)

Gustavo Basso / Wikimedia Commons (CC BY-SA 4.0)
COVID-19 — caused by SARS-CoV-2, a coronavirus that emerged in Wuhan, China in late 2019 and was declared a pandemic by the WHO on March 11, 2020 — has killed approximately seven million people in confirmed deaths as of 2024, with excess mortality estimates suggesting total deaths attributable to the pandemic of 15 to 20 million globally. It is the most consequential pandemic since the 1918 influenza pandemic and the first pandemic in history to occur in the era of real-time genomic sequencing, social media, and mRNA vaccine technology.
SARS-CoV-2 spread via respiratory aerosols and droplets, primarily in indoor settings with poor ventilation, and exhibited pre-symptomatic and asymptomatic transmission that made case-based containment strategies (which had worked for SARS in 2003) largely ineffective. The virus's combination of high transmissibility, a significant proportion of asymptomatic infections, and a long incubation period produced sustained community transmission in every country to which it spread.
The acute pandemic phase ended through the combination of widespread vaccination (multiple vaccines developed within a year of the pandemic's emergence, using mRNA technology tested for decades but never previously deployed at scale in an approved vaccine), mass infection producing population immunity, and the evolution of the virus toward less severe dominant variants (Omicron and its descendants). COVID-19 has not ended in the sense that SARS ended — the virus continues to circulate globally, causing significant illness and some death — but it has transitioned from a pandemic with acute healthcare system strain to a pattern of endemic circulation that most health systems now manage without emergency measures.
Pathogen: SARS-CoV-2 (coronavirus). Death toll: approximately 7 million confirmed; 15–20 million estimated. How it transitioned: mass vaccination; population immunity through infection; viral evolution to lower-severity variants.
Polio (1916–1979 in the US; ongoing globally)
_(7184148409)-1920x1440.jpg)
The U.S. Food and Drug Administration / Wikimedia Commons
Poliomyelitis — caused by poliovirus, an enterovirus spread primarily through the fecal-oral route via contaminated water and food — paralyzed tens of thousands of children annually in the United States during the epidemic years of the 20th century and caused global paralysis and death on a scale that made it one of the most feared diseases of the era. The 1952 US polio epidemic — the worst in American history — paralyzed 21,269 people and killed 3,145.
Polio's specific epidemiological paradox was the role of improved sanitation in amplifying epidemics: in unsanitary conditions, most children were exposed to poliovirus as infants, when maternal antibodies still provided some protection and clinical illness was usually mild. As sanitation improved in the early 20th century, first exposure shifted to older children and adults, whose immune response to poliovirus was more severe, producing more cases of paralysis. The epidemic of paralytic polio was, in part, a consequence of the success of 19th-century sanitation reforms.
The development of the Salk inactivated polio vaccine in 1955 and the Sabin oral polio vaccine in 1961 produced rapid declines in polio incidence in vaccinated populations. The United States eliminated endemic polio by 1979. The Global Polio Eradication Initiative, launched in 1988, has reduced wild poliovirus cases globally by more than 99.9% — from approximately 350,000 cases per year in 1988 to single digits annually by the early 2020s. Wild poliovirus type 2 was declared eradicated in 2015; wild poliovirus type 3 in 2019. Wild poliovirus type 1 persists in Pakistan and Afghanistan, making polio one of the closest examples of a near-eradication story still in progress.
Pathogen: Poliovirus. Death toll: hundreds of thousands globally over the epidemic period. How it has been nearly ended: Salk and Sabin vaccines; Global Polio Eradication Initiative; wild type 1 persists in two countries.