
Credit: Canva Images
The question of how long a human life can last — and how much of that ceiling is fixed versus malleable — has occupied scientists for centuries. What has changed in the last decade is the pace of discovery. Advances in genomics, epigenetics, and microbiome science have allowed researchers to move from broad observations about aging populations to granular, molecular-level explanations for why bodies deteriorate and why some individuals seem to slow that process down.
The field of geroscience, which treats aging itself as a biological process that can be studied and potentially modified, has gained serious institutional backing. Longevity research is no longer a fringe pursuit. Major universities, private foundations, and pharmaceutical companies have invested heavily in understanding the cellular and systemic mechanisms of aging, not simply to extend lifespan but to extend healthspan — the number of years a person lives in good health.
Several threads have emerged as especially productive. The discovery that senescent cells — old, damaged cells that stop dividing but refuse to die — accumulate in aging tissues and trigger inflammation has opened an entirely new line of research. The role of the gut microbiome in immune function, cognition, and metabolic health has become clearer and more complex at the same time. Epigenetic clocks, which measure biological age rather than chronological age, have given researchers a new tool for tracking how lifestyle factors affect the pace of aging at the cellular level.
Sleep, once treated as a passive state, is now understood as one of the most active and consequential processes for brain health and longevity. The importance of muscle mass — not just cardiovascular fitness — has been reframed as a central pillar of healthy aging. And the relationship between chronic low-grade inflammation and nearly every major age-related disease has been quantified more precisely than before.
This is not a field defined by simple answers or straightforward prescriptions. Much of what has been learned raises as many questions as it resolves. But the accumulation of findings over the past ten years represents the most substantive shift in scientific thinking about aging in generations. What follows is a breakdown of 20 of the most consequential things researchers have learned.
1 / 20
Credit: Sangharsh Lohakare / Pexels
For most of human history, age meant one thing: how many years had passed since you were born. Researchers now have tools to measure something more precise and more predictive — biological age, which reflects the actual condition of your cells and tissues rather than how long you have been alive.
The most widely used methods rely on epigenetic clocks, which measure chemical modifications to DNA called methylation marks. These marks accumulate in patterns that correlate with aging, and they can be read from a blood sample. Researchers including Steve Horvath at UCLA developed the first generation of these clocks in the early 2010s, and the technology has been refined substantially since. Newer versions, sometimes called "second-generation" or "pace of aging" clocks, are better at predicting disease risk and mortality than simply counting years.
What makes this distinction consequential is what it reveals about variability. Two people who are both 60 years old can have biological ages that differ by a decade or more. One person's cells may show methylation patterns consistent with a 50-year-old; another's may look more like a 70-year-old. This isn't random. Biological age tracks closely with lifestyle factors — smoking, obesity, chronic stress, physical inactivity, and poor sleep all tend to accelerate it. Exercise, good nutrition, and not smoking tend to slow it.
The clocks have also helped researchers establish that biological aging is not a steady, linear process. A study published in Nature Medicine in 2019, based on analysis of nearly 3,000 proteins in blood plasma, found that aging appeared to accelerate in waves — with notable shifts occurring around age 34, 60, and 78. This suggests that aging has internal structure, with distinct phases rather than a smooth decline.
From a practical standpoint, biological age testing is becoming commercially available, though the clinical utility of consumer-grade tests is still debated. More importantly for research, these clocks have given scientists a way to test whether interventions — drugs, dietary changes, behavioral shifts — actually slow the aging process at the cellular level rather than just improving a single health marker.
The larger implication is that aging is not a fixed destiny. For a given chronological age, biological age can vary widely, and that variation is at least partly within human influence.
2 / 20
Credit: National Cancer Institute / Unsplash
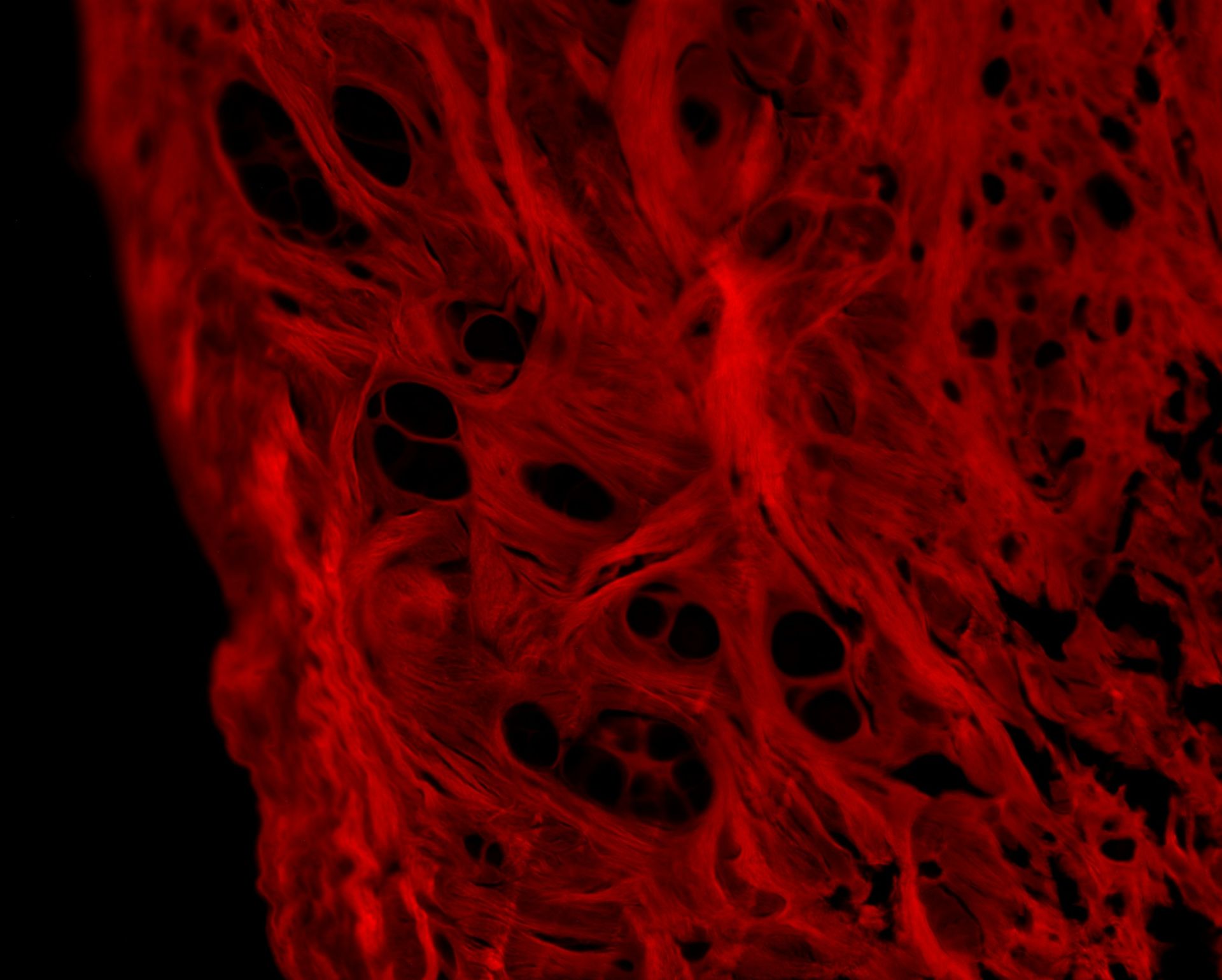
Inside an aging body, some cells stop dividing but do not die. They linger in tissues, metabolically active, secreting a cocktail of inflammatory molecules that damage neighboring cells and contribute to a range of age-related diseases. These cells are called senescent cells, and understanding their role in aging has been one of the most productive research threads of the last decade.
The phenomenon of cellular senescence was first described in the 1960s, when Leonard Hayflick showed that human cells in culture stop dividing after a certain number of replications. But the significance of senescent cells in living organisms — and their role in disease — was not fully appreciated until more recently. Work by Judith Campisi at the Buck Institute for Research on Aging and others helped establish that senescent cells accumulate with age and that what they secrete, a phenomenon called the senescence-associated secretory phenotype, or SASP, actively promotes chronic inflammation.
That chronic inflammation, sometimes called "inflammaging," is now understood to be a key driver of conditions including heart disease, type 2 diabetes, Alzheimer's disease, osteoarthritis, and certain cancers. Senescent cells are not the only source of inflammaging, but they are one of the most tractable targets because they are, in principle, removable.
The proof of concept came in a landmark 2011 study published in Nature. Researchers led by Jan van Deursen at the Mayo Clinic showed that selectively clearing senescent cells in mice delayed the onset of multiple age-related conditions — cataracts, muscle wasting, fat loss — and extended the healthy lifespan of the animals. The effect was seen even when the cells were cleared in middle-aged mice, not just young ones.
This led to the development of a class of drugs called senolytics, which are designed to selectively kill senescent cells. The combination of dasatinib (a cancer drug) and quercetin (a plant flavonoid) has been the most studied senolytic cocktail in early human trials. Results from small clinical trials have been published for conditions including lung fibrosis and diabetic kidney disease, with some promising signs of reduced senescent cell burden and inflammation.
The field is still early, and human evidence remains limited. But the conceptual shift — that removing specific categories of dysfunctional cells could meaningfully slow aging — has opened a genuinely new therapeutic avenue.
3 / 20
Credit: Google DeepMind / Unsplash
The human gut contains trillions of microorganisms — bacteria, fungi, viruses, and archaea — that collectively perform functions no single organ could manage alone. They help digest food, produce vitamins, regulate the immune system, and communicate with the brain via the vagus nerve. Over the last decade, research has clarified how profoundly this microbial ecosystem changes with age and how much those changes matter for health outcomes.
In younger adults, the gut microbiome tends to be diverse, with a wide variety of species competing and cooperating in a relatively stable ecosystem. With age, that diversity tends to decline. Beneficial bacteria — particularly members of the Bifidobacterium and Lactobacillus genera, as well as butyrate-producing species like Faecalibacterium prausnitzii — become less abundant. Bacteria associated with inflammation tend to increase. The barrier function of the gut lining can also weaken with age, a phenomenon sometimes called "leaky gut," which allows bacterial fragments to enter the bloodstream and trigger immune responses.
A 2021 study published in Nature Metabolism analyzed gut microbiome data from more than 9,000 people across multiple age cohorts and found that the degree of microbial uniqueness — how different a person's microbiome was from the population average — was positively associated with longevity. People who lived into their 90s tended to have more distinctive, individualized microbiomes than those who died younger. This does not establish causation, but it points to microbiome dynamics as a meaningful signal of overall health.
The connection between the gut microbiome and the brain — sometimes called the gut-brain axis — has also received significant research attention. Gut bacteria produce neurotransmitters and neuroactive compounds, including serotonin precursors and gamma-aminobutyric acid. Changes in the microbiome have been associated with mood disorders, cognitive decline, and even neurodegenerative diseases like Parkinson's, which is increasingly understood to have a gut component.
Interventions that support microbiome diversity — including dietary fiber from a wide variety of plant sources, fermented foods, and reduced antibiotic use — have shown modest but consistent benefits in several studies. The microbiome is not a simple on-off switch for aging, but it is increasingly clear that it is an active participant in the process.
4 / 20

Credit: cottonbro studio / Pexels
For decades, body weight and body mass index were the dominant metrics used to assess health risk in clinical settings. The last decade of research has substantially complicated that picture. What appears to matter more than total weight — and more than BMI — is the ratio of muscle to fat, and in particular the preservation of skeletal muscle mass as people age.
The condition of age-related muscle loss is called sarcopenia, from the Greek for "poverty of flesh." It begins as early as the late 30s, with adults losing roughly 3 to 5 percent of muscle mass per decade after age 30 if no active steps are taken to counter it. The rate accelerates after age 60. By the time a person reaches their 80s, sarcopenia is common and often severe, contributing to falls, fractures, loss of mobility, and dependence on others for daily activities.
But the significance of muscle mass extends beyond physical function. Muscle is metabolically active tissue. It is the primary site of glucose disposal, meaning it plays a central role in maintaining blood sugar regulation and insulin sensitivity. People with more muscle mass tend to have better metabolic health, lower rates of type 2 diabetes, and faster recovery from illness or injury. Muscle also serves as a protein reserve that the body draws on during acute illness — a resource that becomes critically important in the context of major surgery, infection, or cancer treatment.
Research published in the American Journal of Medicine and other journals has found that muscle mass is a more reliable predictor of mortality risk in older adults than BMI. Among people over 55, those in the lowest quartile for muscle index had significantly higher mortality rates than those with higher muscle mass, regardless of their body fat percentage.
The implications for how people approach fitness are significant. Cardiorespiratory fitness remains important, but resistance training — lifting weights, using resistance bands, or any exercise that places load on muscles — is now understood as essential for healthy aging, not optional. Building and preserving muscle requires consistent mechanical stress on the tissue, combined with adequate protein intake, and these two factors together are among the most evidence-supported tools available for extending healthspan.
5 / 20
Credit: Canva Images
Sleep has long been understood as restorative, but the mechanism behind that restoration was poorly understood. The last decade produced a discovery that clarified it substantially. The brain has its own waste-clearance system — called the glymphatic system — and it operates almost exclusively during sleep.
The glymphatic system was described in a 2013 paper by Maiken Nedergaard and colleagues at the University of Rochester. It works through cerebrospinal fluid, which flows through channels that surround blood vessels in the brain. During sleep, particularly deep non-REM sleep, these channels appear to expand, allowing cerebrospinal fluid to flush through brain tissue and clear out metabolic waste products. Among the waste products cleared is amyloid-beta, one of the proteins that accumulates in the brains of people with Alzheimer's disease.
In animal studies, sleep deprivation caused measurable accumulation of amyloid-beta and tau — another protein implicated in neurodegeneration — within hours. A 2017 study published in JAMA Neurology found that healthy middle-aged adults who reported poor sleep quality had higher levels of amyloid-beta in their brains than those who slept well. A 2021 study in Nature Communications, drawing on data from nearly 8,000 people followed over 25 years, found that consistently sleeping six hours or fewer per night at age 50 was associated with a 30 percent higher risk of developing dementia later in life.
The relationship between sleep and cognitive aging is not limited to dementia risk. Chronic sleep deprivation accelerates biological aging as measured by epigenetic clocks, impairs immune function, elevates cortisol, and disrupts the regulation of hunger hormones. Even a single night of inadequate sleep produces measurable impairments in attention, emotional regulation, and metabolic function.
What this body of work has established is that sleep is not a passive state the body falls into when there is nothing else to do. It is an active, carefully orchestrated biological process during which critical maintenance occurs. For longevity research specifically, sleep quality — not just duration — has emerged as a variable that tracks closely with multiple aging outcomes.
6 / 20
Credit: Tayfun Dikmen, Unsplash
Inflammation is the body's primary defense mechanism against infection and injury. Acutely, it is essential and protective. The problem with aging is that the inflammatory response becomes chronically activated at a low level — present even in the absence of infection or injury, and never fully switched off. Researchers have come to call this state "inflammaging," and its connection to the major diseases of aging is now well established.
The list of conditions linked to chronic low-grade inflammation is extensive. Cardiovascular disease, type 2 diabetes, Alzheimer's disease, Parkinson's disease, certain cancers, osteoarthritis, chronic kidney disease, and depression all involve inflammatory mechanisms. In many cases, elevated levels of inflammatory markers — including C-reactive protein, interleukin-6, and tumor necrosis factor-alpha — are measurable years before a diagnosis, suggesting that inflammation is not simply a consequence of disease but a contributing cause.
Several sources feed inflammaging. Senescent cells, as described elsewhere, are one. The gut microbiome is another — a dysbiotic microbiome can allow bacterial fragments to enter the bloodstream and trigger immune activity. Visceral fat tissue is itself an inflammatory organ, secreting cytokines that maintain systemic inflammation. The declining ability of aging immune cells to resolve inflammation — a process that requires specific signaling pathways — is also a factor.
One of the more precise contributions of recent research has been the identification of the NLRP3 inflammasome, a molecular complex in immune cells that acts as a sensor and activator of inflammation. The NLRP3 inflammasome becomes more active with age and is implicated in a range of age-related conditions. Drugs and compounds that inhibit it, including some already approved for other uses, are being investigated for broader anti-aging applications.
The practical upshot is that interventions known to reduce chronic inflammation — sustained exercise, a diet high in vegetables and fiber and low in refined carbohydrates and ultra-processed foods, adequate sleep, and not smoking — work through mechanisms that are now understood at the molecular level. The lifestyle advice has not changed dramatically, but the reasoning behind it has become substantially more specific.
7 / 20

Credit: National Cancer Institute / Unsplash
Blood is not just a transport medium for oxygen and nutrients. It is an information-dense biological fluid containing thousands of proteins, metabolites, and other molecules that reflect the state of nearly every organ system in the body. Over the last decade, researchers have developed increasingly powerful tools to read that information as a measure of biological aging.
A study published in Nature Medicine in 2019 analyzed levels of nearly 3,000 proteins in the blood plasma of more than 4,000 individuals ranging in age from 18 to 95. The researchers identified around 1,400 proteins that changed significantly with age and were able to build a predictive model of biological age based on just 373 of them. Crucially, the protein-based biological age diverged from chronological age in patterns that correlated with health outcomes — people whose protein profiles suggested they were biologically older than their years tended to have worse health.
A separate line of research has explored what happens when old blood is diluted or replaced with young blood. In animal experiments, transfusing young blood into old mice produced improvements in muscle function, brain activity, and other markers of aging. The research group led by Tony Wyss-Coray at Stanford identified GDF11 and other factors as potentially responsible for some of these effects, though subsequent work made the picture more complicated and certain early findings have not fully replicated. What the research confirmed, however, is that circulating factors in blood play an active role in regulating how aging progresses throughout the body.
Another development has been the identification of proteins in blood that appear to accelerate aging. Research from the Conboy lab at UC Berkeley found that a protein called TGF-beta becomes elevated in old blood and contributes to cognitive decline and muscle deterioration in aging animals. When its signaling was blocked, some age-related changes were reversed.
Taken together, this body of work positions blood composition as both a readout of biological age and a potential lever for modifying it — a framing that was largely theoretical a decade ago but is now being actively pursued in clinical trials.
8 / 20

Credit: Sami Aksu / Pexels
The observation that reducing caloric intake extends the lifespan of organisms from yeast to mice has been replicated hundreds of times since the 1930s. What the last decade has clarified is the molecular machinery behind that effect — and what that means for humans, who are unlikely to adopt severe caloric restriction as a lifestyle practice.
The most important pathway is TOR, or target of rapamycin. TOR is a protein kinase that acts as a master regulator of cell growth and metabolism. When nutrients are abundant, TOR is active and cells prioritize growth and protein synthesis. When nutrients are scarce, TOR is suppressed, and cells shift into maintenance mode — repairing damage, clearing debris, and slowing down processes associated with aging. The drug rapamycin, which inhibits TOR, has extended lifespan in multiple animal models, including mice, even when given late in life. It remains one of the most replicated pharmacological longevity interventions in animal research.
Intermittent fasting and time-restricted eating have attracted attention as practical approximations of caloric restriction. Animal research has found benefits from restricting feeding to specific time windows, independent of total calorie intake — the timing itself appears to matter because it aligns feeding with circadian rhythms and creates periods of fasting during which TOR is suppressed and cellular cleanup processes are activated. Human trials have produced more mixed results, with some studies finding metabolic benefits and others showing the advantage largely disappears when calorie intake is controlled.
Autophagy, the process by which cells break down and recycle damaged components, is one of the key mechanisms activated during fasting and caloric restriction. Named in the Nobel Prize-winning work of Yoshinori Ohsumi, autophagy declines with age, contributing to the accumulation of cellular debris. Fasting reliably activates autophagy in animal models, and there is evidence for the same effect in humans, though the magnitude and duration required to produce meaningful benefits is not yet established.
What this research suggests is that the timing and pattern of eating — not just the content — influences aging pathways in ways that are mechanistically understood, even if the optimal human protocol remains an open question.
9 / 20
-1920x1080.jpg)
Credit: Viktor Mindt / Unsplash
Nicotinamide adenine dinucleotide, or NAD+, is a coenzyme found in every cell in the body. It plays a fundamental role in energy metabolism — transferring electrons during cellular respiration — and also acts as a signaling molecule that activates a class of enzymes called sirtuins, which regulate DNA repair, gene expression, and stress responses. NAD+ levels decline substantially with age, and that decline is now understood to contribute to multiple hallmarks of the aging process.
By the time a person reaches their 50s, their NAD+ levels are roughly half what they were in their 20s. This matters because the enzymes that depend on NAD+ — including the sirtuins and a DNA repair enzyme called PARP1 — become less active as NAD+ drops. Cells become less efficient at repairing DNA damage, regulating inflammation, and maintaining mitochondrial function, all of which are relevant to both aging and age-related disease.
Research in animal models has shown that restoring NAD+ levels — either through precursor supplementation or by blocking the enzymes that consume it — can reverse some aspects of cellular aging. Studies led by David Sinclair at Harvard Medical School showed that supplementing mice with NMN (nicotinamide mononucleotide), a precursor to NAD+, improved muscle function, energy metabolism, and some markers of aging. Similar effects were seen with NR (nicotinamide riboside).
Human trials with NR and NMN have confirmed that these precursors do raise NAD+ levels in blood and tissues. Whether that elevation translates into meaningful health or longevity benefits in humans is still being tested. Several small trials have reported improvements in muscle function, blood pressure, and insulin sensitivity in specific populations, but large, definitive clinical trials have not yet been completed.
The sirtuins activated by NAD+ are also the target of resveratrol, a compound found in red wine, which attracted significant attention in the 2000s. The evidence for resveratrol's effects in humans has proven weaker than animal studies suggested, but the sirtuin pathway itself remains a legitimate research target, with better-characterized compounds in development.
10 / 20
Credit: National Cancer Institute / Unsplash
Mitochondria — the organelles responsible for generating most of the cell's energy supply through ATP production — are central to aging in ways that have become clearer over the last decade. Mitochondrial function declines with age, and that decline feeds into multiple other hallmarks of aging, including oxidative stress, inflammation, cellular senescence, and loss of stem cell activity.
Mitochondria are unusual among organelles in that they carry their own DNA, a remnant of their origin as free-living bacteria that were incorporated into early eukaryotic cells more than a billion years ago. Mitochondrial DNA is more vulnerable to damage than nuclear DNA because it lacks many of the repair mechanisms present in the nucleus and sits in close proximity to the reactive oxygen species generated during energy production. Over time, mitochondrial DNA accumulates mutations that impair the efficiency of the electron transport chain, the molecular machinery through which ATP is generated.
When mitochondria are damaged or dysfunctional, they are normally cleared through a quality-control process called mitophagy, in which the cell degrades and recycles defective mitochondria. This process is closely related to general autophagy and is also suppressed in aging cells. The accumulation of dysfunctional mitochondria creates a vicious cycle: damaged mitochondria generate more reactive oxygen species, which cause more DNA damage, which further impairs mitochondrial function.
Exercise is the most effective known intervention for maintaining mitochondrial health. Aerobic exercise stimulates the production of new mitochondria through a process called mitochondrial biogenesis, which is regulated in part by a molecule called PGC-1alpha. High-intensity interval training has been found to be particularly effective at stimulating mitochondrial biogenesis, including in older adults. A 2017 study published in Cell Metabolism found that high-intensity interval training reversed many age-related cellular changes in skeletal muscle in older adults, with some of the most striking improvements seen in mitochondrial function and protein synthesis.
11 / 20
-1920x1080.jpg)
Credit: Sangharsh Lohakare / Unsplash
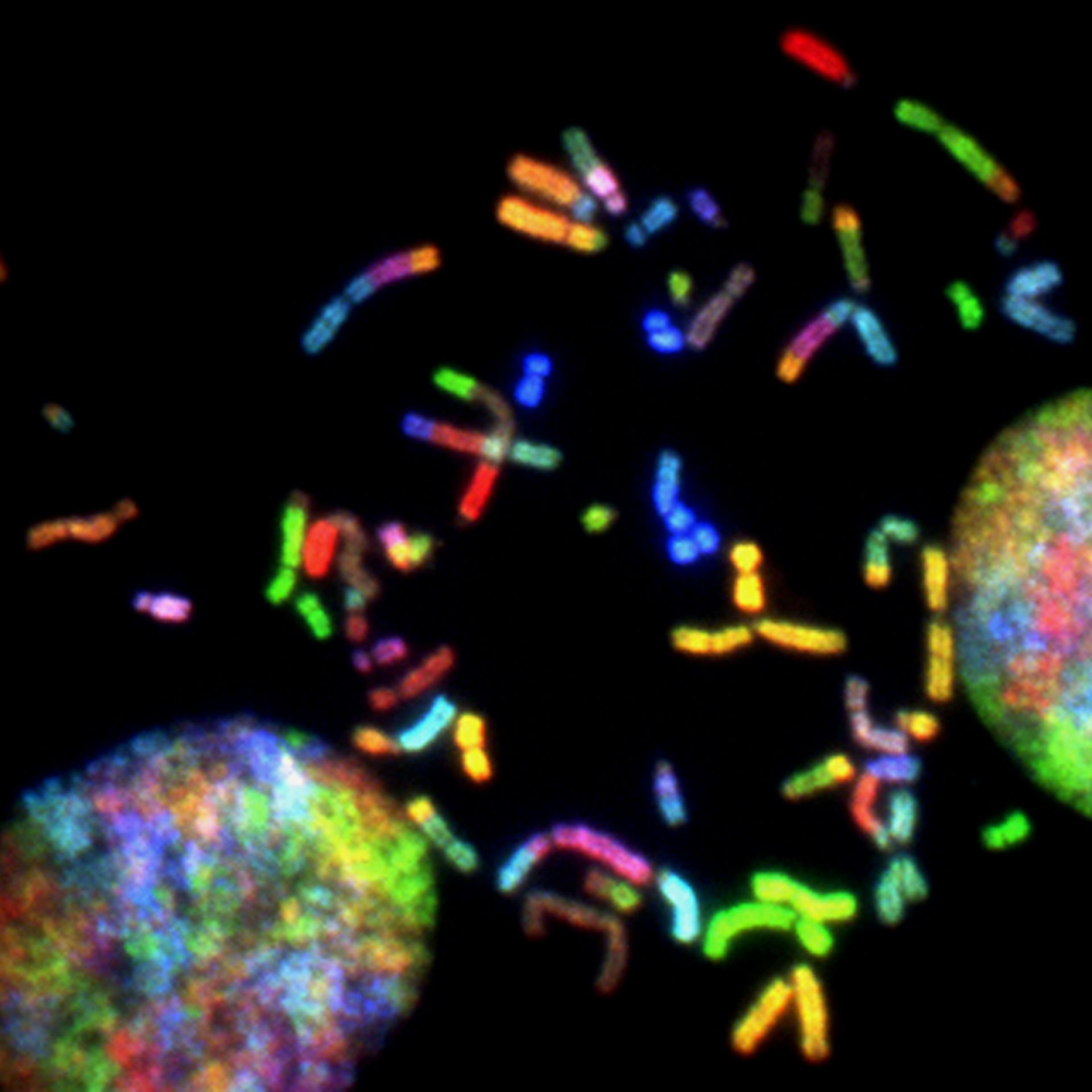
Telomeres are the protective caps at the ends of chromosomes, comparable in function to the plastic tips on shoelaces. Each time a cell divides, telomeres shorten slightly. When they become critically short, the cell enters senescence or undergoes programmed death. Because of this, telomere length has been used as a proxy for biological age, and shorter telomeres have been associated with a higher risk of age-related diseases and earlier death in population studies.
The relationship between telomeres and aging dominated popular discussions of longevity for much of the 2000s and early 2010s. Since then, the picture has become more nuanced. Telomere length is indeed associated with health outcomes, but the size of the effect in humans is smaller than early enthusiasm suggested, and telomere length explains only a modest fraction of the variation in biological aging.
Several factors influence telomere attrition rate. Chronic psychological stress — particularly early-life adversity — accelerates telomere shortening. Elizabeth Blackburn and Elissa Epel's research on telomeres and stress, which helped earn Blackburn a share of the 2009 Nobel Prize in Physiology or Medicine, established that the enzyme telomerase, which rebuilds telomere length, is suppressed under chronic stress conditions.
Smoking is one of the most reliably documented accelerants of telomere shortening, with studies consistently finding shorter telomeres in smokers compared to non-smokers of the same age. Obesity, sedentary behavior, and high levels of oxidative stress are also associated with faster attrition.
The nuance that research has added is that telomere length is better understood as a marker of cumulative cellular wear-and-tear than as a direct cause of aging in most tissues. Some tissues — such as intestinal epithelium, which turns over rapidly — depend heavily on telomere maintenance, and mutations in telomerase genes cause severe premature aging syndromes. But in other tissues, and in healthy aging in general, telomere dynamics are one factor among many rather than the primary driver. Researchers who focused on restoring telomere length as a longevity strategy have found the results in animal models to be more complicated than the original theory suggested.
13 / 20

Credit: Gustavo Fring / Pexels
Beyond social connection, the broader category of psychological wellbeing — including sense of purpose, emotional regulation, optimism, and life satisfaction — has emerged as a significant predictor of longevity in longitudinal research. The mechanisms are not fully resolved, but the epidemiological pattern is consistent enough to have shifted thinking in geroscience.
The concept of ikigai — a Japanese term roughly translating to "reason for being" — has entered Western health discussions partly because of research attention to Okinawa, one of the world's so-called Blue Zones, where exceptional longevity has historically been documented. Whether ikigai itself is causally protective, or whether it is a proxy for other factors common in communities with social cohesion and traditional lifestyles, remains an open question. But the association between reported sense of purpose and health outcomes has been found in other populations and settings.
A study published in JAMA Psychiatry in 2019 followed more than 6,000 adults over four years and found that those with a stronger sense of purpose had lower rates of sleep disturbance, reduced risk of cardiovascular events, and slower decline in physical function. The relationship held after controlling for depression, social engagement, and baseline health status. Other research has found associations between higher purpose scores and lower rates of Alzheimer's disease, lower inflammatory biomarkers, and better metabolic health.
Optimism has been studied separately. Research published in PNAS in 2019, drawing on data from two large cohorts including the Women's Health Initiative, found that people in the top quartile of optimism lived on average 11 to 15 percent longer than those in the bottom quartile, and were significantly more likely to reach age 85. The effect remained after controlling for depression, health behaviors, and socioeconomic factors.
None of this implies that attitudes can cure disease or that positive thinking overrides biology. What it suggests is that psychological states have physiological correlates — in inflammation, in stress hormone regulation, in immune function — that accumulate over decades and contribute meaningfully to health outcomes.
14 / 20

Credit: Anna Shvets / Pexels
Among the measurable indicators of longevity risk, cardiorespiratory fitness — the ability of the heart, lungs, and circulatory system to deliver oxygen to working muscles during sustained exercise — has emerged in research as one of the most powerful predictors available. This finding has accumulated across multiple large cohort studies and has led some researchers to argue that fitness should be treated as a clinical vital sign.
The most commonly used measure of cardiorespiratory fitness is VO2 max, which quantifies the maximum rate at which the body can consume oxygen during intense exercise. VO2 max declines with age at roughly 10 percent per decade after age 30 in sedentary individuals, and the rate of decline is substantially slower in people who maintain aerobic exercise. Higher VO2 max is associated with lower rates of cardiovascular disease, cancer, metabolic disease, and all-cause mortality.
A study published in JAMA Network Open in 2018, based on data from more than 122,000 patients who underwent treadmill testing, found that low cardiorespiratory fitness was associated with a higher risk of mortality than smoking, hypertension, or type 2 diabetes. The association between fitness and mortality was continuous — each incremental improvement in fitness level corresponded to a meaningful reduction in mortality risk, with the greatest gains coming from moving out of the lowest fitness category.
Exercise physiologist Peter Attia and others have argued that peak aerobic capacity is among the most important variables to maintain during midlife precisely because it declines with age and because the baseline from which it declines determines how much functional capacity a person retains in old age. A 50-year-old with a VO2 max of 50 ml/kg/min will, at the same rate of decline, have substantially more functional capacity at 80 than someone who was sedentary at 50.
The relevant exercise for maintaining VO2 max includes sustained aerobic activity at moderate and high intensities — running, cycling, swimming, rowing, and similar activities. Zone 2 training, performed at a conversational pace for extended durations, has received particular attention for its role in mitochondrial health and metabolic efficiency, and is increasingly recommended as a foundational component of longevity-oriented exercise.
15 / 20

Credit: Daniela Elena Tentis / Pexels
After decades of research organized around specific nutrients — fat, carbohydrates, cholesterol, antioxidants, omega-3s — the scientific consensus has shifted toward an emphasis on overall dietary patterns rather than individual components. The evidence now consistently shows that the quality and composition of the whole diet predicts aging outcomes better than any single nutrient or food category in isolation.
The Mediterranean diet has the largest body of supporting evidence for longevity. It is characterized by high intake of vegetables, legumes, whole grains, fish, olive oil, and nuts, with moderate wine consumption and low intake of red meat and ultra-processed foods. A major clinical trial published in the New England England Journal of Medicine in 2013 — the PREDIMED trial, later corrected and republished — found that participants assigned to a Mediterranean diet supplemented with olive oil or nuts had a significantly lower risk of major cardiovascular events than those assigned to a low-fat diet.
Ultra-processed foods have received increasing research attention as a category associated with accelerated aging and elevated disease risk. A study published in The BMJ in 2019, following more than 100,000 French adults, found that a 10 percent increase in the proportion of ultra-processed foods in the diet was associated with a 14 percent higher risk of all-cause mortality. Ultra-processed foods displace more nutrient-dense options, alter the gut microbiome, and expose consumers to higher levels of food additives whose long-term effects are not well characterized.
Protein intake in older adults has been revised upward in recent research consensus. Older adults require more dietary protein than younger adults to achieve the same rates of muscle protein synthesis, partly because of a phenomenon called "anabolic resistance" — the reduced efficiency of muscle tissue in responding to protein intake. Earlier dietary guidelines recommending 0.8 grams of protein per kilogram of body weight daily are now widely regarded as insufficient for older adults seeking to preserve muscle mass. Many researchers focused on healthy aging recommend 1.2 to 1.6 grams per kilogram of body weight per day for older individuals.
16 / 20

Credit: www.kaboompics.com / Pexels
Stress has always been recognized as detrimental to health, but the last decade of research has provided a more precise framework for understanding how it accumulates and damages the body over time. The concept of allostatic load — the cumulative biological cost of chronic stress and adversity — has moved from a theoretical construct to a measurable composite score with clinical relevance.
Allostatic load is calculated from a battery of biomarkers that capture the state of multiple physiological systems: cardiovascular function, metabolic regulation, immune activity, and neuroendocrine signaling. High allostatic load scores are associated with faster biological aging, higher rates of cardiovascular disease, cognitive decline, and increased mortality. The concept is useful because it captures the wear-and-tear of chronic stress across systems, rather than focusing on any single marker.
What research has clarified is that the timing and duration of stress exposures matters enormously. Early-life adversity — childhood poverty, neglect, abuse, or chronic instability — has effects on stress response systems that persist into adulthood and midlife. The Adverse Childhood Experiences (ACEs) studies, which have been replicated and extended substantially over the last decade, have established that high ACE scores predict higher rates of nearly every major age-related disease later in life, through mechanisms including epigenetic changes to the stress response system that can persist for decades.
The glucocorticoid system — centered on cortisol, the body's primary stress hormone — is one of the main pathways through which chronic stress accelerates aging. Elevated cortisol over time is associated with accelerated telomere shortening, impaired immune function, reduced hippocampal volume, and higher blood glucose. Cortisol suppresses immune activity in ways that are protective in the short term but destructive when maintained chronically.
Interventions that reduce allostatic load — including meditation, exercise, therapy, and improvements in social and economic circumstances — have been shown to measurably reduce inflammatory and neuroendocrine markers over time. Exercise in particular operates on multiple stress-related pathways simultaneously, which is one reason it consistently appears across research as among the highest-impact longevity behaviors.
17 / 20

Credit: Google DeepMind / Pexels
A widely held assumption — reinforced by the popular appeal of genetics — is that lifespan is largely inherited. The actual evidence, accumulated across decades of twin studies and genome-wide association research, paints a different picture. Genetics account for roughly 20 to 30 percent of the variation in human lifespan. The remaining 70 to 80 percent reflects environment, behavior, and chance.
Twin studies are the most direct way to separate genetic from environmental contributions to longevity. A large study using Danish twin registry data, published in Human Genetics, found that the heritability of lifespan was approximately 26 percent for men and 23 percent for women. When exceptional longevity — defined as living past 90 or 100 — is studied specifically, heritability estimates are somewhat higher, suggesting that genetic factors play a larger role at the extreme end of the distribution. But even for centenarians, the genetic contribution is modest compared to what the concept of "longevity genes" implies in popular discourse.
Genome-wide association studies have identified variants associated with longevity, including variants near the APOE gene (which also affects Alzheimer's risk), FOXO3 (associated with exceptional longevity in multiple populations), and CETP (involved in cholesterol metabolism). But these variants individually explain tiny fractions of lifespan variation. There is no single "longevity gene" — the genetic architecture of long life is highly polygenic, meaning it involves many genes each with small effects.
The practical implication is that genetic predispositions are not destiny in either direction. A person with a genetic profile associated with higher cardiovascular risk can substantially modify that risk through behavior. Conversely, a genetic profile associated with longevity is no guarantee of it in the presence of chronic smoking, obesity, or sedentary lifestyle. Epigenetics — how gene expression is modified by environment and behavior without changing the underlying DNA sequence — has emerged as the layer connecting genes to outcomes, and it is a layer substantially within human influence.
18 / 20
Credit: National Cancer Institute / Unsplash
The aging of the immune system — a process called immunosenescence — is one of the reasons older adults are more vulnerable to infectious disease, respond less well to vaccines, and have higher rates of cancer. But it also feeds back into the broader aging process through chronic inflammation, because an aging immune system loses some of its capacity to resolve inflammation once it has been initiated.
The immune system undergoes several well-characterized changes with age. The thymus, a gland behind the breastbone that produces T cells — the cells responsible for targeted immune responses — begins to shrink during puberty and is largely replaced by fat tissue by middle age. This thymic involution reduces the production of naive T cells, meaning the immune system gradually loses its ability to mount responses to new pathogens. The population of memory T cells, which recognize previously encountered pathogens, takes up a larger share of the immune repertoire, which is protective in some ways but limits flexibility.
Natural killer cells, which provide rapid innate immune responses against infected and cancerous cells, decline in both number and function with age. The proportion of pro-inflammatory immune cells tends to increase. And the capacity of immune cells to resolve inflammation — to switch off inflammatory signals once a threat has been cleared — diminishes.
Greg Fahy and colleagues published a small but notable clinical trial in 2019 in Aging Cell, known as the TRIIM trial. The trial tested a combination of human growth hormone, DHEA, and metformin in a small group of healthy older men and found evidence of thymic regeneration and rejuvenation of the epigenetic age of immune cells. Epigenetic aging appeared to reverse by an average of 2.5 years during the trial, though the sample size was small and the findings require replication.
Exercise and lifestyle factors influence immune aging substantially. Regular aerobic exercise is associated with preservation of thymic output, better vaccine responses, and lower levels of inflammatory markers in older adults. The mechanisms include improved circulation, reduced visceral fat, and the anti-inflammatory effects of regular physical activity.
19 / 20

Credit: Canva Images
The concept of "Blue Zones" — geographic regions where people live measurably longer than average — entered mainstream culture through the work of Dan Buettner and his collaboration with demographers and scientists in the 2000s. The five originally identified zones were Sardinia, Italy; Okinawa, Japan; Loma Linda, California; Nicoya Peninsula, Costa Rica; and Ikaria, Greece. Over the last decade, the research surrounding these places has deepened and also been scrutinized more carefully.
The common factors identified across these populations have been widely cited: plant-heavy diets, regular low-intensity physical activity embedded in daily life (rather than structured gym workouts), strong social cohesion, sense of purpose, moderate caloric intake, and low rates of smoking. These factors align well with what laboratory and epidemiological research has independently established about longevity.
Subsequent analysis has added complexity. A 2023 paper by Saul Newman at Oxford raised methodological concerns about some Blue Zone longevity data, pointing to inconsistencies in record-keeping and age verification in regions where civil registry systems were historically unreliable. The paper argued that some of the extreme longevity attributed to these populations may partly reflect poor data quality rather than genuine biological advantage. This was a legitimate methodological critique, though it did not negate the broader patterns of healthy aging behaviors observed in these communities.
The Okinawan experience has been complicated by generational change. The traditional Okinawan diet — low in calories, high in sweet potatoes and vegetables, with modest amounts of fish and pork — has been largely displaced by a modern diet following the post-World War II period, and Okinawa's longevity advantage among younger cohorts has diminished substantially. This is a natural experiment in how rapidly dietary and lifestyle change can shift population health trajectories.
What the Blue Zones research offers is not a formula to replicate but a set of consistent patterns that align with mechanistic science. No single factor — not a specific food, not a specific practice — explains the longevity advantage. The patterns point to a cluster of behaviors and social conditions operating together over a lifetime.
20 / 20

Credit: Canva Images
Among pharmacological interventions tested in animal models, rapamycin stands out for the breadth and consistency of its effects on aging and lifespan. It is currently the only drug that has extended lifespan in mammals when given late in life — a finding that has been replicated by multiple independent labs and that continues to generate significant research activity.
Rapamycin was originally developed as an immunosuppressant drug for organ transplant recipients. It works by inhibiting the TOR pathway — the same nutrient-sensing pathway that caloric restriction suppresses — which shifts cells from growth mode into maintenance and repair mode. By mimicking aspects of caloric restriction at the molecular level, rapamycin appears to slow several hallmarks of aging simultaneously.
In a landmark study published in Nature in 2009, three independent research groups fed rapamycin to mice beginning at 600 days of age — roughly equivalent to 60 years in humans — and found that it extended median and maximum lifespan. The effect was seen in both male and female mice, which is notable because some longevity interventions in animals show sex-specific results. Subsequent studies found that rapamycin improved cardiac function, delayed cancer onset, preserved immune function, improved cognitive function, and reduced age-related inflammation in aged mice.
No large randomized controlled trial has tested rapamycin for longevity in healthy humans. The drug carries real risks — it is an immunosuppressant and is associated with elevated blood glucose, impaired wound healing, and increased infection susceptibility at the doses used in transplant medicine. Researchers studying its potential anti-aging applications have proposed that much lower, intermittently dosed regimens might preserve the benefits while reducing side effects. Several clinical trials using modified rapamycin analogs or low-dose intermittent protocols are underway.
The significance of rapamycin in longevity research is less about its current clinical readiness than about what it confirms: that the rate of biological aging in mammals is not fixed, and that single pharmacological interventions can alter it in measurable ways. That finding has reshaped what the field believes is possible.
12 / 20
Social connection predicts health as strongly as physical factors
Credit: Yaroslav Shuraev / Pexels
One of the more counterintuitive findings to gain traction in longevity research over the last decade is that the quality and quantity of a person's social relationships predicts their health and lifespan as reliably as many physical factors. This is not folk wisdom dressed up in data — it is a finding that has emerged from large, prospective studies and that holds up even after controlling for other variables.
The Harvard Study of Adult Development, which has followed a cohort of men since 1938, published updated findings in recent years showing that relationship quality — not income, not fame, not productivity — was the strongest predictor of health and happiness in late life. Men who reported high relationship satisfaction in their 50s were the healthiest in their 80s. Those who reported loneliness showed faster cognitive decline and died younger.
Isolation and loneliness operate on the body through several biological pathways. Chronic loneliness activates the body's threat-response systems in a way similar to chronic stress, elevating cortisol, suppressing immune function, and increasing inflammatory markers. Julianne Holt-Lunstad at Brigham Young University conducted a meta-analysis of 148 studies — covering more than 300,000 people — and found that social isolation was associated with a 29 percent higher risk of mortality and loneliness with a 26 percent higher risk.
Sleep is one of the mediating pathways. Lonely individuals show worse sleep quality and less restorative deep sleep, which then feeds into the cognitive and metabolic consequences of poor sleep described elsewhere in this list. Loneliness also correlates with higher rates of unhealthy behaviors — poorer diet, less exercise, higher alcohol consumption — though these behavioral factors do not fully account for the biological effect.
The public health implications have become more visible since the COVID-19 pandemic, which created a natural experiment in mass social isolation. Research on the health consequences of that period continues, but preliminary findings have reinforced the idea that social connection is not a luxury component of a healthy life but a core biological need with measurable consequences when unmet.